Urban Testing and Games with Models, 5/14/19
Maybe the most-notable thing about today’s COVID-19 data release for Rhode Island was the big increase in the number of tests conducted. Out of 3,679 tests (up from 2,683 the day before) 181 were positive, for a positive rate of 5%. If we’re going to see an increase from the slight reopening of Governor Raimondo’s Phase One, it should begin in the next few days… although the amount of loosening was so minimal, some skepticism that we’ll see an increase is justified.
Another interesting angle that has been in the news, lately, has been the differences in percentage positive tests in urban community clinics:
As statewide testing numbers dip — only 8% of the test results reported Tuesday from all sites were positive, according to R.I. Health Department data — Gov. Gina Raimondo has sounded increasingly optimistic about her plans to cautiously reopen the state in phases. But the urban neighborhood testing sites, which serve lower-income and higher-risk patients, are seeing positive results that are more than double or triple the statewide percentage.
One big factor is (as readers of this site will know) population density:
The Blackstone Valley Community Health Center has tested nearly 1,000 patients in Central Falls, Pawtucket and Cumberland in the past six weeks, with 24% testing positive, double the statewide rate.
“It is safe to state that the positivity rate is always positively correlated with population density,” said Ray Lavoie, the executive director. “Central Falls and Pawtucket, as two of the most densely populated cities in Rhode Island, are proof of this.”
When I asked on Twitter about any differences in testing standards, Common Cause’s John Marion told me that the urban community clinics are more likely to have professionals doing the tests, compared with other sites where, he says, sometimes parents are being permitted to stick the swabs into their own children’s noses. Understandably, they may tend not to shove them deep enough.
In response to one of my earlier Games with Models posts, one person on Twitter criticized me as follows:
Minimize the threat all you want so you can go out to eat. The fact is in the poorest communities in the state the numbers are skyrocketing
This perspective offers an opportunity to think about how we should be responding to the threat of the virus. If it’s true that the numbers have been skyrocketing in poor areas under our shut-down regime, then that’s evidence that our approach has been incorrect, or at least insufficient — that it hasn’t been working.
Of course, we could put the screws to our economy even more, but that would risk losing whatever willingness currently have to comply. An alternate view would be that it makes no sense to shut down everybody for problem affecting people in a limited area. Consider this: If the numbers in urban areas are disproportionately high, that means that everywhere else, they have to be even lower.
Closing down the economy hurts everybody. If a family has some members who can’t work, it is more important for the others to work. The last thing they should do is not to work as a statement of solidarity. That’s how we ought to look at our economy statewide and nationally. Protect the vulnerable. Place restrictions where they’re actually needed. And give everybody maximal freedom to assess their own situations and make their own judgments. At the same time, figuring out some way to help those who do have to limit their activities would be reasonable.
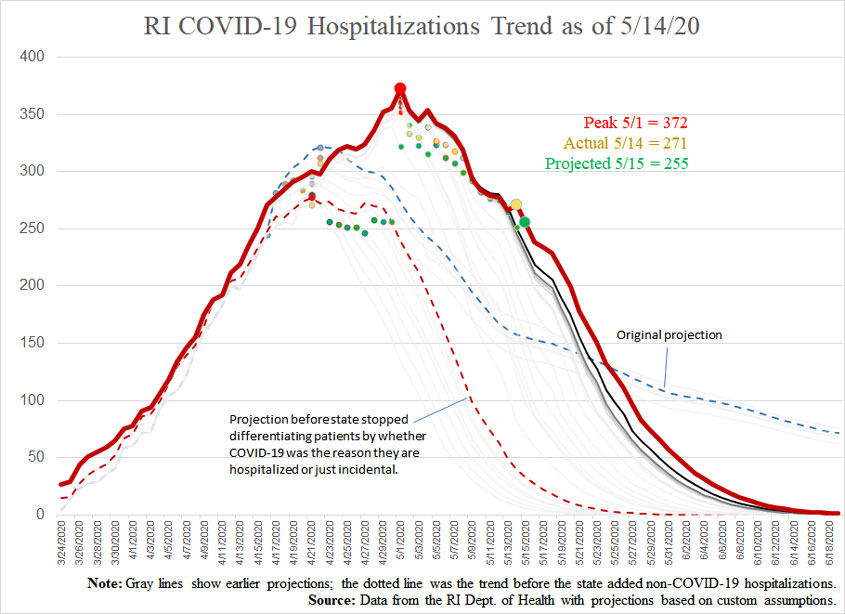
In the meantime, the numbers continue to improve. A small uptick in the number of Rhode Islanders hospitalized with COVID-19 cannot yet be called a trend, and it resulted mainly from a large downward revision of yesterday’s number.
Projections versus actuals (date reported):
- Cases:
- Projection for 5/14: 11,972
- Actual for 5/14: 12,016
- Projection for 5/15: 12,140
- Hospitalizations:
- Projection for 5/14: 251
- Actual for 5/14: 271
- Projection for 5/15: 255
- Deaths:
- Projection for 5/14: 467
- Actual for 5/14: 468
- Projection for 5/15: 473


