Games with Models, April 22 Data
As data is corrected and Rhode Island rounds the peak for COVID-19 cases and hospitalizations, it may be time to adjust the projection methodology.
As data is corrected and Rhode Island rounds the peak for COVID-19 cases and hospitalizations, it may be time to adjust the projection methodology.
The emerging question when it comes to the daily data releases for COVID-19 in Rhode Island continues to be: which metric should we be watching? Today, the number of cases continued to outstrip my prediction as did, tragically, the number deaths. However, the number of hospitalizations, which is the focus of my model, went down one from yesterday and was, therefore, substantially lower than my prediction.
The reason the model I developed shows what looks like an upward correction and the predicted decline spreading out has to do with the number of cases. The rate of growth is slowing, but not as quickly as it had been, which means there are more “active” cases than expected, and that’s the foundation of my hospitalization predictions. (By the way, here’s the original post of this series, with my methodology.)
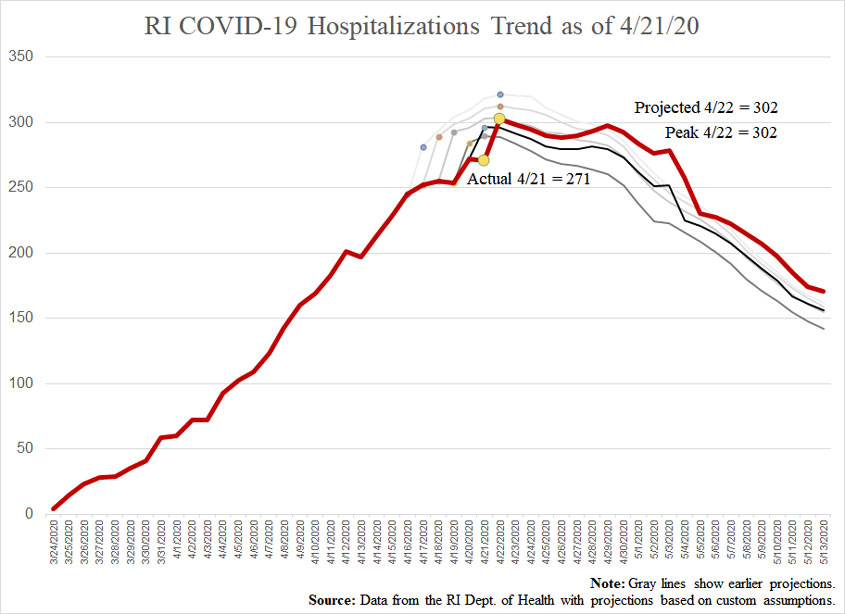
The three key metrics now look as follows:
The level of power Governor Raimondo is claiming for herself is huge, and it is noticeable in subtle ways. For example, in an article on GoLocal about how she’s had her hair done even as Rhode Islanders are prevented from doing the same, the governor tells “hairdressers, barbers, gig economy workers” to file for unemployment “until I can find a way to get you open safely.”
Notice that it’s all up to her. She is going to find a way. She is going to tell you when you can work again. If she is going to do that, she should give Rhode Islanders detailed information and data about how she is making decisions so we can judge for ourselves whether what she is concluding is reasonable or ridiculous.
On March 16, the White House issued “15 Days to Slow the Spread” guidelines.
On March 28, Governor Gina Raimondo issues a stay-at-home order for Rhode Island.
At that time, the IHME’s model projected 100,000-240,000 deaths from COVID-19.
At that time, the goal of the lockdown was to “flatten the curve” of the disease so as to not overwhelm our hospitals with cases. Note, critically, that reducing the overall number of cases was NOT part of this goal but simply to spread them out.
Since March 28, the IHME’s projections have collapsed and the new projection for COVID fatalities is 60,000.
Since March 28, the results of numerous COVID-19 anti-body surveys have come in.
My weekly call-in on John DePetro’s WNRI 1380 AM/95.1 FM show, for April 20, included talk about:
I’ll be on again Monday, April 27, at 12:00 p.m. on WNRI 1380 AM and I-95.1 FM.
Of course, because the trend of this weekend was a leveling-off of COVID-19 hospitalizations, it was tempting to think we’d already hit the peak, and today’s increase to 272 people in the hospital proves that wasn’t so. Nonetheless, the increase was still less than my model had predicted.
(It bears repeating that these projections are based entirely on recent trends, so there isn’t any assessment of how viruses spread.)
For today, the model had projected 284 hospitalizations, and the actual number turned out to be 272.
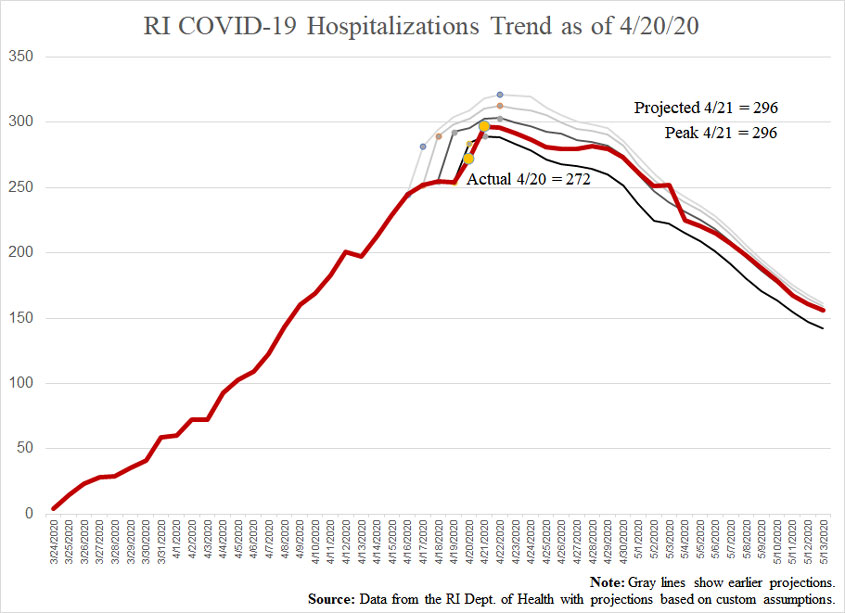
Here’s how the one-day predictions stacked up to reality and where they’re going next:
Naturally, to the extent that cases can follow a different trend than hospitalizations and deaths, it’s great to see the latter two going down. Increased testing would tend to mean we’re recording more cases leaning toward the less-serious side and would also tend to make the model overestimate for hospitalizations and deaths.
These trends move the projected peak of active cases to 4,082 tomorrow, with 1,067 Rhode Islanders’ having recovered.
Hopefully the slight downturn in COVID-19 hospitalizations in Rhode Island reported today will mark this as the start of the down slope in infections. The model I’ve been following suggests we’ll have a couple more days of increases, but that trend is affected by the fact that I’m still capturing a few days of large increases in my averages.
As it was, for today, I’d projected 293 hospitalizations, but the reported number was actually down one, to 254. The following chart reflects the updated projections.
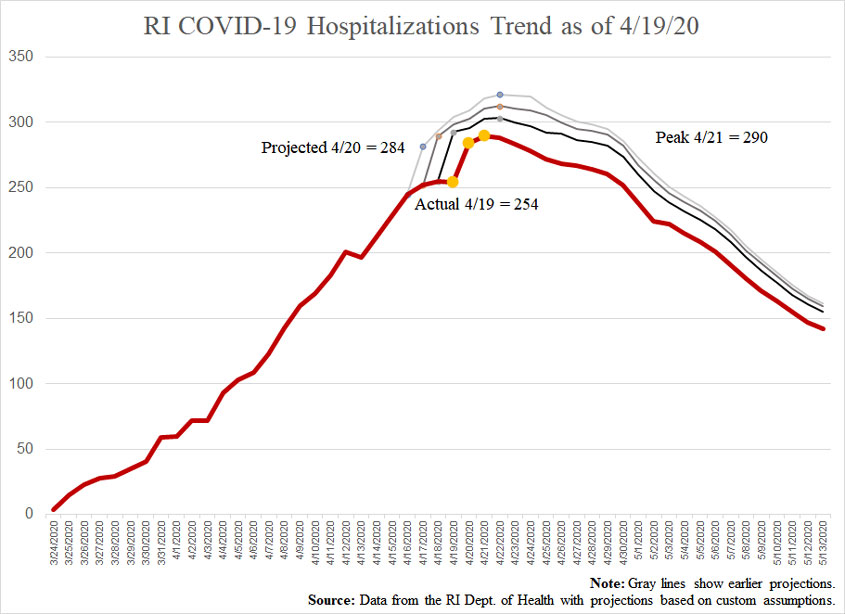
Broadening to the three key metrics we’re all watching, this is how we’re looking:
It is more than disappointing to see the numbers of deaths coming in higher than projected even as other metrics slow down. That could just be the fact that the disease worked its way into some high-risk populations, so recovery will lag.
Another important point as the governor starts talking about what we’ll have to see before she’ll permit us to get back to something closer to regular life: If she bases her judgment on the number of actual cases, that’s the wrong measure. Total cases are going to keep going up for the foreseeable future (although current trends put them hitting a plateau in mid-May if we don’t loosen restrictions.
This is why it is important for people in power to start talking about active cases. When it comes to the spread of the disease, somebody who has had the disease and recovered will almost certainly be a walking stopper of the disease. It is amazing that nobody in Rhode Island is talking about how many have recovered.
My model has active cases peaking at 3,902 on Tuesday, with an underlying 1,065 people having recovered. The question the governor should be encouraging us to consider and discuss among ourselves (this being a government of, by, and for the people, you know) is what should be tolerable.
If we focus our energies on protecting at-risk people, then we can start to open up for everybody else and loosen or tighten our behavior to stay within an acceptable margin for hospitalizations. For example, if COVID-19 hospitalizations fall between 150-200 people at any given time, with only a few deaths attributable to the disease each day, is that too many, or should the acceptable threshold be higher?
Keep in mind that our current solution is creating a breeding ground for social diseases and deaths associated with those.
I noticed something interesting today. Thus far, Governor Raimondo’s daily briefings on the coronavirus have produced a flurry of social media posts and articles emphasizing three metrics: cases, hospitalizations, and deaths. Over recent weeks, some journalists have said that hospitalizations is the key trend to watch, and when the governor gave a little bit of transparency into the data behind her decision-making, she released a chart projecting… yes… hospitalizations.
Well, while it may only be a temporary reprieve, the increase in hospitalizations has slowed way down in the past couple days, and suddenly that is no longer the subject of concern. Some local reporters have even switched to emphasizing only cases and deaths.
But that’s not how informing the public about trends is supposed to go. We shouldn’t follow a metric until it stops being interesting and then switch to something more topical.
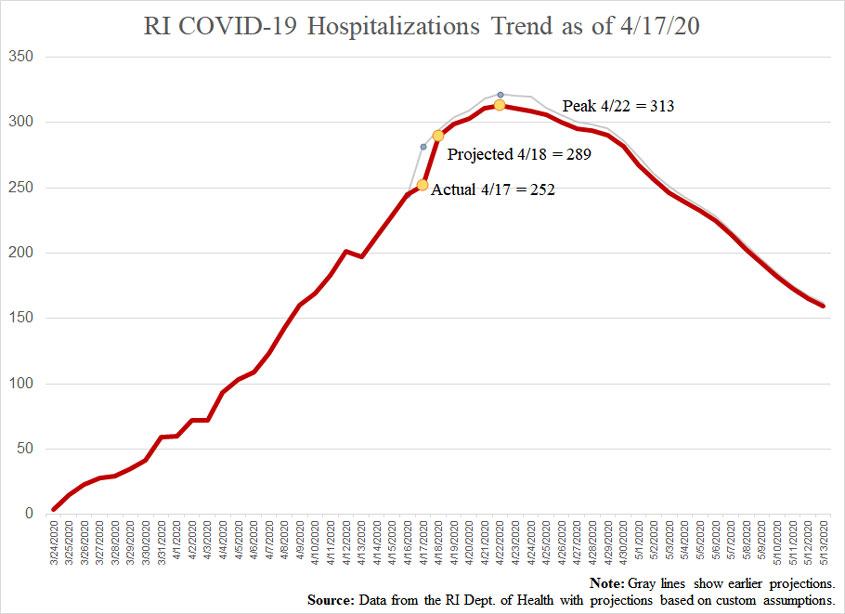
So, to keep up the series of posts projecting hospitalizations in Rhode Island, here’s the chart based on today’s new data. Yesterday’s projection was for us to have 289 people in the hospital today, and the reported number was actually 255. It would be reasonable to suggest that the projection for tomorrow, of 293, is once again too high, but this model measures trends over the past week so as to be less volatile.
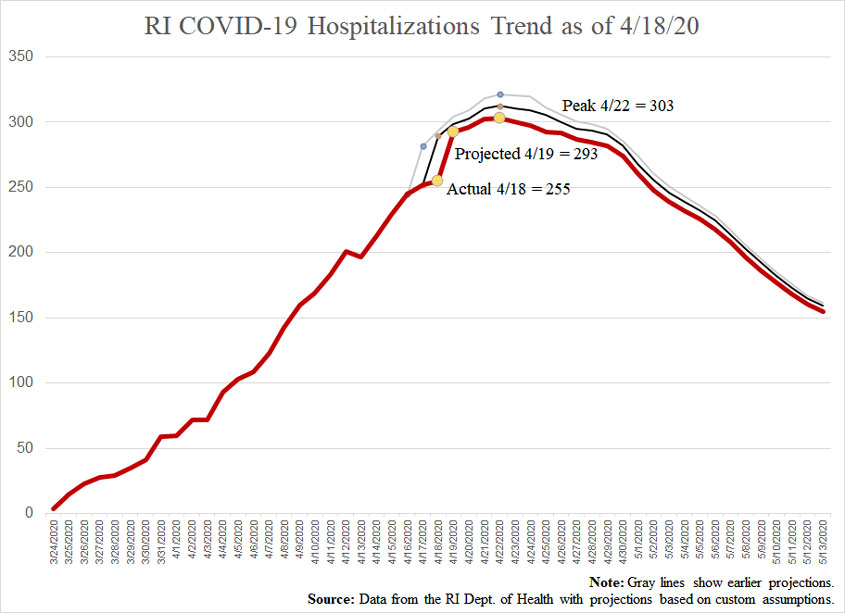
Based on the new numbers, the model suggests that tomorrow’s report will be:
Unfortunately, although hospitalizations have been coming in below estimates, cases and deaths have been a little higher than projected.
Turning back to hospitalizations, the three models currently suggest they’ll peak as follows:
It occurs to me that daily comparisons of COVID-19 predictions versus reported numbers would be more useful if the model is adjusted soon after the daily data dump, so I’ll put up two of these posts today. This one adjusts my model for yesterday’s numbers, and this afternoon, I’ll put up another based on whatever news the governor reports.
For April 17, I had predicted 282 total hospitalizations (as in, people currently in the hospital). The reported number was 252. Adjusting for the reported numbers of cases and hospitalizations produces the following:
For the record, the underlying predictions that produce this line suggest that today the governor will announce:
As of this writing, the three models I’m tracking suggest the following change in hospitalizations:
Rhode Islanders can make decisions as adults and don’t need Constitutionally suspect impositions from our chief executive.
The various models projecting RI hospitalizations based on COVID-19 create the opportunity for data hobbyists to try their hands at predictive modeling. Here’s mine.
Governor Raimondo announced that she was going to give Rhode Islanders more transparency into the data that she’s using to make decisions about the extent of our freedom during the COVID-19 wave, and even the RI Center for Freedom & Prosperity commended the intention. What Rhode Islanders actually got, however, wasn’t much transparency, but rather, an incomplete chart of a single metric without any description of the methodology.
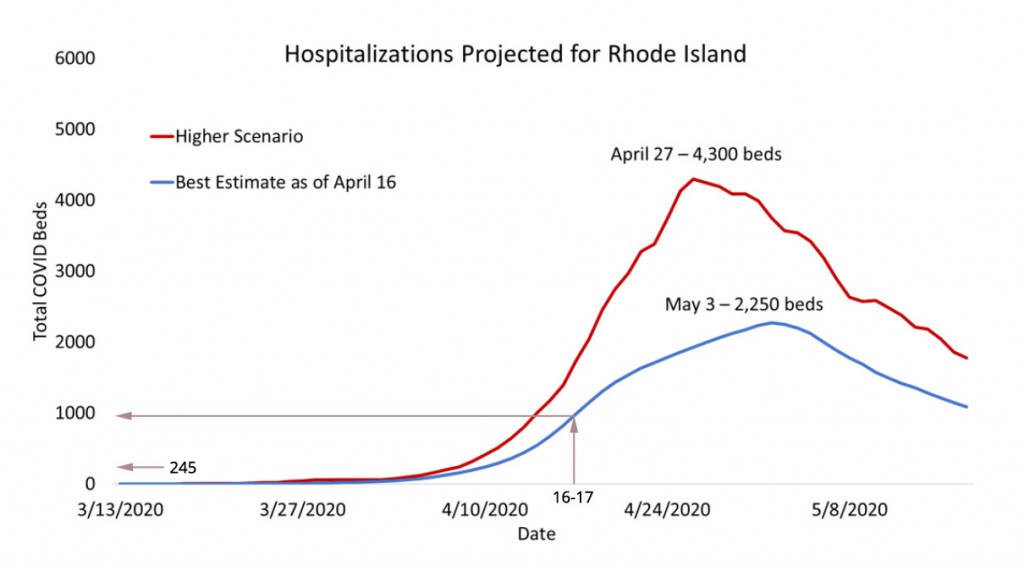
What’s conspicuously missing from this chart is a “lower scenario.” See, for example, the IHME model for Rhode Island, which has a worst-case scenario of 4,386 hospital beds needed on May 6, a “projection” of 942 on May 2, and a best-case scenario that has us already beginning to see a reduction.
Rhode Islanders shouldn’t hope for that outcome, but given how high the IHME’s projections have proven so far versus reality and how much higher the governor’s estimates apparently are than theirs, we should expect many fewer hospitalizations than she’s saying. It’s difficult not to conclude that she’s painting a bleak picture so as to mislead Rhode Islanders into better compliance with her directives. That’s especially true if you notice that the governor’s “best estimate” line appears to show nearly 1,000 people in the hospital today, when the actual number is 245.
As I’ve been saying, we are adults and deserve accurate information. We are not children who need an elected mother to coax us with phrases like, “I need you to be brave.”
Again, rates of growth have been slowing. Seventeen days ago, hospitalizations were increasing around 25% every day. That’s down to about 7% now. At the same time, the increase of total cases has been slowing, as has the percentage of all cases who are going to the hospital.
The question the governor apparently didn’t answer (and that apparently nobody asked) is why we should expect these trends to reverse such that the number of hospitalizations will be nine times higher in 17 days than it is right now. That would be an average of 15% increase every day. Why should we expect the rate of hospitalization to accelerate like that?
Maybe there’s some data out there that would give us reason to expect such an outcome, but we should know what it is, and the people who gave Raimondo her chart should be able to explain it to her.
Some real data and some rough calculations would allow the public to judge for ourselves how much risk we’re willing to bear and where public resources can best be deployed.
Looked at more closely, the Imperial College epidemiological model whose frightening projections set our current reaction in motion
Rhode Island’s hospitals and healthcare systems are disproportionally represented on Fitch’s downgrade list and so disproportionately endangered by the onerous and dangerously archaic COVID-19 lockdown.
If models projecting the hospitalizations and deaths in Rhode Island from COVID-19 keep being revised down, they’ll start to get into the range at which deaths from our response are a larger number.
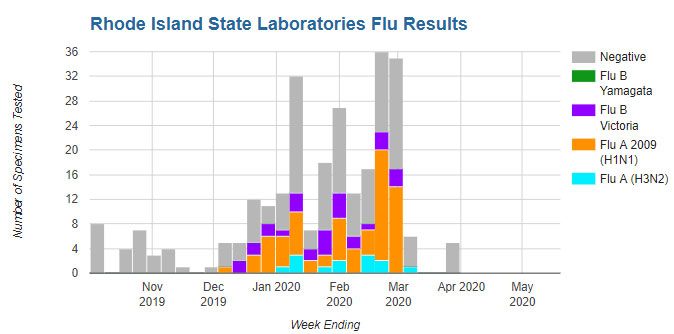
One of the persistent questions surrounding this outbreak of the COVID-19 coronavirus is whether all of the people who had a bout of some mysterious flu-like illness in the two months or so before the world really started to pay attention to the disease have already had it. Writing on her Facebook page, Lisa Daft made the excellent observation that Rhode Island saw “a lot of negative flu tests this winter.”
The chart she displays comes from the RI Dept. of Health’s Influenza Surveillance page, which currently offers the following, with the gray sections representing tests that came back negative for the flu, presumably despite flu-like symptoms:
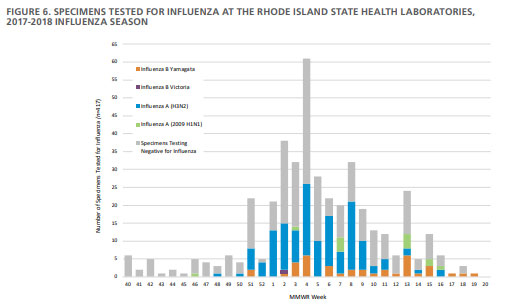
Can the number of those negative results actually be showing us early COVID-19 infections? Possibly, but finding the same chart in the last few years of the Dept. of Health’s annual report suggests these results aren’t actually unusual (2016, 2017, 2018, 2019). Here’s the one from two years ago:
These trends are consistent with national experience. The following chart shows the number of flu-negative tests for the United States from October 2015 through January 2020, as reported by the World Health Organization:
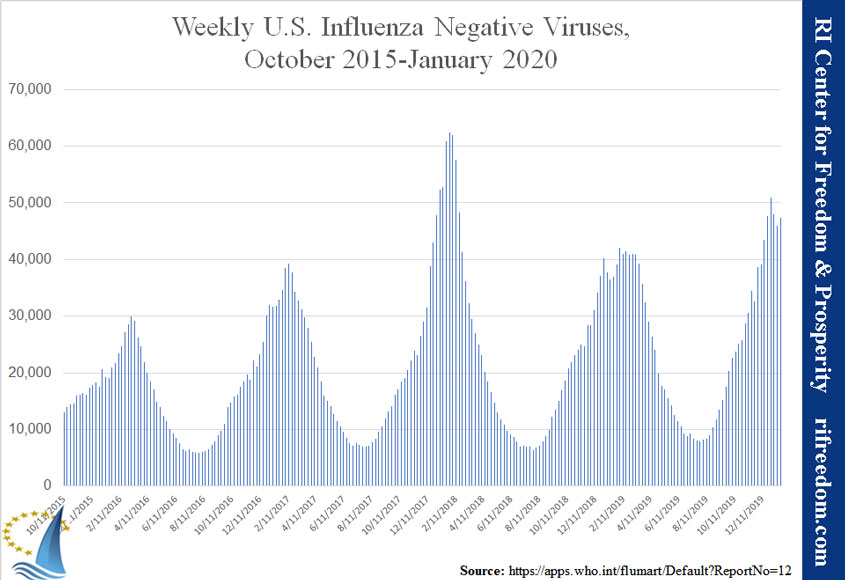
So, while negative tests during this flu season look like they’re going to prove to have been higher than average, they aren’t unusual, and this hasn’t been the worst year on record for negative tests. Of course, that doesn’t mean the strange illnesses so many people have reported were not COVID-19. Every year, the number of negative tests could be accounted for by something different, ranging from the amount of attention the media is paying to the flu to the severity of the flu season (making people more inclined to get tested) to an outbreak of some virus that is never identified.
The next question to answer would be how many deaths occur each year due to mysterious illnesses that initially present as the flu.
The disconnect between the warnings of government officials and the experiences of the people could make it more difficult to manage the COVID-19 pandemic and its aftermath.
Here’s some encouraging news out of London:
The British government is just “days” away from releasing 3.5 million self-administered finger prick tests that could prove a game-changer in easing the economic fallout from the coronavirus pandemic.
The tests will likely be stocked in retailers like Boots, a major pharmacy chain in the United Kingdom, and available to order online via Amazon, however the first stage of the rollout will be reserved for doctors, nurses and other essential workers.
At first, the tests would be held for critical personnel, but as more are produced, they’ll be available to the general public.
The article emphasizes that people who have the antibodies and are therefore inoculated can get back to work (and, implicitly, economically productive play). Of course, knowing that they haven’t yet built up an immunity will also help people make decisions about how isolated to make themselves.
This news speaks to a question many families have surely had upon hearing that Massachusetts Governor Charlie Baker has extended the ban on in-person schooling to May 4. Isn’t that an unnecessarily pessimistic step? Going forward, a vaccine would be the gold standard relief innovation, but that isn’t the only thing to watch for. Means of treating the effects of the virus (not only for individuals, but also for hospitals to handle large numbers of cases) are also in the works, and broad availability of tests for live infections and immunity would be hugely helpful in managing the epidemic.
The entire world is focused on this disease. We’ve already inculcated a sense of the importance of hygiene and social distancing, as well as a practice of self evaluation for symptoms. If we improve our knowledge about who is infected and who is immune, while we reduce the worst effects for individuals and hospitals or limit the populations who might experience them, restrictions could ease sooner than expected.
Of course, in a situation like this, we shouldn’t count on such outcomes, but we should leave open the possibility.
My weekly call-in on John DePetro’s WNRI 1380 AM/95.1 FM show, for March 23, included talk about:
I’ll be on again Monday, March 30, at 12:00 p.m. on WNRI 1380 AM and I-95.1 FM.
A Rhode Island family has a child with a disease that requires pretty significant daily treatments and an increased concern about illnesses like the flu. After receiving the diagnosis, they increased their household emphasis on hygiene, cleanliness, exercise, and health and battled with tricky questions about longevity and quality of life.
When do you pull a child out of school? What sort of activities can you no longer do? Water parks might definitely be out, per the doctor, but what about trampoline parks and that sort of thing? That is for each family to decide.
This year, the child is in a grade that traditionally takes an extended class field trip, which has been a source of anxiety for the parents for months, or even years. The early weeks of attention to COVID-19 put a sharper point on that anxiety, and it was looking more and more likely that they would have to speak the difficult “no.”
In such circumstances, it might be natural for parents to feel a little bit of guilty relief when they don’t have to say, “no,” because the event itself is canceled. But circumstances have moved well past that. The final, decisive end of hope for the trip was closure of the century-old Rhode Island travel company that handled the arrangements from its Cumberland office.
The company opened its doors in 1926. It survived the Great Depression, World War II, the stagflation of the 1970s, the dot-com bubble, and the Great Recession. In the face of COVID-19, the announcement on the website of Conway Tours gives the impression that the owners have no plans to re-open or try to start things up again when the wave of this virus has passed.
Without doubt, travel agencies are uniquely vulnerable to the recession that we now face, but the survival of other businesses and industries that live a bit farther from the cliff’s edge will depend on how we, as a society, respond to the crisis. It’s still too early to know what the best response is, right now, but we have to remain mindful that none of our reactions is without a trade-off.
Recent public debates have renewed over the old conflict between security and freedom, but the question is deeper than that. Civilizations have to make decisions that balance longevity and quality of life, too, because every life begins with a diagnosis of its end. That is nothing new, and nothing unique to any given family.
As the federal government and states’ governors decide how much to clamp down on free motion, they should keep in mind the geographic specificity of coronavirus cases.
Take away the scary studies based on China and Italy and frightening “whatifs,” and it’s difficult to conclude that the economic harm has thus far proven worthwhile, leaving citizens to figure out what the thresholds should be.
We can’t let the most-extreme cases and simplistic online simulations hustle us past a reasonable assessment of our current situation the lessons of history.
My weekly call-in on John DePetro’s WNRI 1380 AM/95.1 FM show, for March 16, included talk about:
I’ll be on again Monday, March 23, at 12:00 p.m. on WNRI 1380 AM and I-95.1 FM.
This bit of a letter from a young doctor puts a spotlight on one of the weaknesses of our modern culture. Noting that healthcare workers are still going to be needed no matter what happens with this virus, he asks:
How can we be proactive about protecting our healthcare workers? To start, we need to consider protecting our older colleagues and those with certain preexisting medical conditions. We may even need to decide that only young and healthy doctors and nurses should be triaging and caring for these patients. I’m in. But is this discriminatory or putting too much risk on the young? I’m not sure.
Step out of our times for a moment, and this is an astonishing thing to read. Not that long ago, it used to be expected that people would sacrifice for others. Young people, in particular young men, would take risks for the whole community where strength and resilience were needed. Heretical as it may be to acknowledge, this is so true that we seem to have evolved around the principle.
Yes, maybe that increased risk came with the compensation of some privileges and cultural encouragement, but trying to distribute such things without the prejudices of the past doesn’t have to mean discarding the ability to differentiate.
A society that doesn’t inspire its people to sacrifice will not last, and a grievance culture characterized by identity politics will not inspire anybody.
As never-let-a-PANIC-go-to-waste grips the country, we’ve been hearing a lot of insistence that the epidemic proves the need for government-run healthcare. Typically, this is merely offered as a Twitter-sized assertion, so there isn’t much specific to argue with. (One suspects that’s by design.)
However, the talk about how our challenge is to keep the incidents within our health system’s capacity rang a bell: specifically, the talk about how the United States has insufficient hospital beds to deal with the potential influx of patients. Here’s the bell, from a House Finance hearing in 2014 on legislation that would have increased the government’s role in Rhode Island health care. This particular speaker is Steve Boyle, who was president of the Greater Cranston Chamber of Commerce, who was advocating for the bill, but the same thing could have been said by any of the supporters:
Boyle says the state needs a “coordinated approach.” “We all know there’s too many hospital beds, but I’m told over and over again that there’s not the political will to close them.”
So, if they didn’t have to worry about “the political will,” the planners at that time would have reduced the number of beds. As it is, our more-socialized health system since Obamacare has overseen a reduction in staffed beds in Rhode Island from 2,535 in August 2012 to 2,424 in August 2018. That 4.4% reduction means 111 fewer spots if there’s a surge.
Now, I’m not saying that the market is always right or that planners are always wrong, but they do take different things into consideration. The market works by finding the value of a particular thing to the society in which it is operating, and that value will naturally adjust for subtler reasons than planners can possibly consider. A culture can remember that its hospital beds filled up at some point in the distant past, while planners might not have the data or might dismiss it.
In times of panic don’t believe people who exploit current circumstances to pretend they would have been able to plan for them if they’d had more power.
Hysteria over the Covid-19 epidemic is missing important considerations that ought to affect our decisions, as well as highlighting changes to our society that should be reevaluated.
My weekly call-in on John DePetro’s WNRI 1380 AM/95.1 FM show, for March 2, included talk about:
I’ll be on again Monday, March 9, at 12:00 p.m. on WNRI 1380 AM and I-95.1 FM.
Guests: Julie Casimiro, State Representative, H-D 31, rep-Casimiro@rilegislature.gov
Camille Vella-Wilkinson, State Representative, H-D 21, rep-vella-wilkinson@rilegislature.gov
Host: Richard August
Topic: Vaping and other pending legislation
Host: Richard August Time: 60 minutes
Representatives Casimiro and Vella-Wilkinson discuss a broad range of pending legislation and other matters, which have their concern. Topics include vaping legislation; a veteran joint oversight committee; pharmacist having birth control prescription authority; reproductive health; firearm legislation; climate control; out of school time learning; early parole for young rehabilitated offenders; military sexual assault trauma; and more. Other matters include the need for a constitutional convention; line item veto; minimum wage; and candidate endorsements.
The campaign manager for President Donald Trump, Brad Parscale, offered a take on the Democrats’ Iowa caucus troubles that probably occurred simultaneously to just about every conservative in the country:
And these are the people who want to run our entire health care system?
A point often gets lost in all the jockeying for control of the American narrative. When we object to this program or that one, conservatives aren’t typically opposing government-driven solutions regardless of whether they’ll work. On the flip side, we also aren’t typically saying that the certainty of a fix can always overcome principled objections based on a philosophy of how government should function.
Rather, the conservative position tends to be that, for any given issue, the trade offs are not sufficiently clear, the benefits are not sufficiently certain, and side effects are so excessively probable that humility should be the underlying principle.
The debacle of the 2020 Iowa caucus should be more proof than anybody needs of this principle. It’s not as if this was the first time Iowa Democrats have caucused, but now (regardless of the reason) there will be lingering doubts about the process, including discord between factions that suspect some sort of political scheme.
To be sure, government and political parties will naturally handle elections-related activities, but they don’t have to handle things like healthcare. Look at experience with the Unified Health Infrastructure Project (UHIP). When bureaucrats committed Rhode Island to the scheme during the Chafee administration, they had wide eyes about “one-stop shopping” for government services. When they rushed ahead with a system that they’d been warned was not ready, no doubt the Raimondo administration was hoping for some sort of PR win. And we got… a debacle.
This isn’t a claim that Democrats are especially incompetent, but that our political system creates incentives and risks that should advise a strong preference for handling society’s challenges through other institutions than government.